
Non-Hodgkin’s lymphoma (NHL) is a heterogeneous group of lymphoid malignancies that most commonly occur in individuals over the age of 60 years. Aggressive (high-grade) subtypes progress rapidly but are potentially curable, whereas indolent (low-grade) subtypes grow more slowly but usually relapse after conventional treatment. The introduction of immunotherapy and its combination with chemotherapy greatly improved remission rates compared with chemotherapy alone in NHL; more recently, the combination of immunotherapy plus yttrium-90 (90Y) or iodine-131 (131I) radiation has shown much greater efficacy than immunotherapy alone and may improve overall survival (OS).
The greatest challenge in NHL is keeping patients in remission once they have responded to therapy. Conventional chemotherapy for indolent lymphoma has a high response rate, but relapses will occur. Although patients may respond to salvage therapy, the duration of remissions decreases progressively. High-dose chemotherapy (HDC) with autologous stem cell transplantation (ASCT) has been shown to increase progression free survival (PFS) with a two-year probability of 70%;1 however, the curative potential in these patients is unclear.
Rationale for Using Yttrium-90–Ibritumomab Tiuxetan in Autologous Stem Cell Transplantation
NHL is inherently radiosensitive, providing a rationale for using radiation to treat lymphomas, and the targeted delivery of radiation directly to tumour sites is better tolerated and more efficient than total body irradiation (TBI). The principles of radiolabelled immunotherapy, which allows targeted delivery of a therapeutic dose of radiation not only to the surface of tumour cells at multiple sites but also to neighbouring deeper cells, have been reviewed extensively in recent publications.2–4 The only radiolabelled immunoconjugates currently approved for the treatment of NHL are 90Y–ibritumomab tiuxetan and 131I–tositumomab (Bexxar®, GlaxoSmithKline, US; only approved in the US), both of which are directed against the CD20 cell surface antigen. 90Y-ibritumomab tiuxetan comprises the anti-CD20 monoclonal antibody ibritumomab, conjugated via the tiuxetan chelator to the pure beta-emitting radioisotope 90Y. It is currently approved for the treatment of adult patients with rituximabrelapsed or -refractory CD20-positive follicular B cell-NHL, and is the only therapy approved for use after rituximab failure. Adverse events with 90Y–ibritumomab tiuxetan are predictable and manageable, with the primary toxicity being transient reversible haematotoxicity, as expected.
No preparative regimens prior to ASCT have been shown to be clearly superior and none has ever been tested in a randomised study. Fractionated TBI has been used in the past, especially in indolent lymphoid malignancies, with encouraging results, but is not recommended for patients above 60 years of age or for those treated with previous radiotherapy.
Therefore, radiolabelled immunotherapy agents such as 90Y– ibritumomab tiuxetan are likely to play an increasingly significant role in ASCT by increasing the efficacy of the conditioning regimen and reducing the relapse risk. Owing to its good tolerability profile, the use of 90Y–ibritumomab tiuxetan at high doses as the sole conditioning agent in place of HDC is also showing promise, and may allow transplantation in patients who cannot tolerate the more aggressive conditioning regimens, such as the elderly or those with co-morbidities (especially cardiovascular disease). The dose-limiting toxicity of radiolabelled immunotherapy is haematotoxicity, which can be circumvented by ASCT and may allow further dose escalation.
Standard-dose Yttrium-90–Ibritumomab Tiuxetan Associated with BEAM Chemotherapy plus Autologous Stem Cell Transplantation
Experience has been gained in several phase II studies with the combination of Zevalin with other conditioning regimens before auto- or allotransplantion.5 The Groupe d’Etude des Lymphomes de l’Adulte (GELA) in France investigated the Z-BEAM conditioning regimen prior to ASTC in patients with relapsing low-grade NHL.6 Radiolabelled immunotherapy 90Y–ibritumomab tiuxetan (Zevalin) is effective in B-cell lymphoma and delivers targeted radiation without TBI toxicity. To take advantage of this antilymphoma effect, a conventional dose of 90Y–ibritumomab tiuxetan 15MBq/kg (maximum total dose 1,200MBq) was given without dosimetry on day -14 before ASCT and combined with a standard-dose BEAM regimen starting at day -7.
The goal of this phase II study was to evaluate the efficacy and toxicity of Z-BEAM. Patients <65 years of age with CD20+ low-grade B-cell lymphoma in first or second relapses, or not achieving complete remission after first-line treatment, were included in the trial. They had to be chemosensitive to prior salvage therapy, have had no more than three lines of treatment and be eligible for ASCT. The primary end-point was to detect a two-year event-free survival (EFS) rate of at least 80%.
Haematological reconstitution was evaluated after transplant and during the first year of follow-up. Between March 2005 and August 2006, 77 patients were included. Patient characteristics at last salvage chemotherapy inclusion were: 68 follicular lymphoma, six marginal zone and one mantle cell plus two transformed histology after pathological review; median age 53 years (range 31–64); follicular lymphoma international prognostic index (FLIPI) low-risk 32, intermediate-risk 20, high-risk 20; and 24 bone marrow involvement. Thirty-nine patients had first relapse, 10 second relapse, 21 partial response (PR), four stable disease and three progressive disease after first-line treatment.
Median delay between first-line therapy and ASCT was 31 months and median delay between last salvage and ASCT was 4.4 months. Response rates before ASCT were complete response (CR) and complete response unconfirmed (CRu) 77%, PR 22% and stable 1%. As first-line treatment, patients received mostly cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP), associated in 29 cases with rituximab. Twenty-nine patients received a second-line chemotherapy with rituximab in 22 cases prior to last salvage chemotherapy; 49 patients after first-line treatment received directly after relapse another line of chemotherapy before ASCT. Overall, among the 77 patients, last salvage chemotherapy regimen included rituximab in 74, and ASCT was performed in 75. The haematological reconstitution after Z-BEAM followed by ASCT in 75 patients was: time to neutrophils >1g/l 12 days (9–35) and time to platelets >20g/l 12 days (range three to 42).
Median number of platelet transfusions was four; median number of red blood cell transfusions was two. Grade 3–4 toxicities were infection (83%), mucositis (47%) and pulmonary (4%). Safety data indicated 35 serious adverse events in 24 patients; these did not appear to significantly differ from those usually seen after ASCT is performed. No cases of toxic death were observed. At weeks 12 and 42 after ASCT, median haemoglobin levels were 11.6g/dl and 11.3g/dl, respectively. Median platelets counts were 111g/l and 148g/l and leukocyte counts were 3.48g/l and 4.80g/l, respectively. After transplant, 91% of the patients were in CR or CRu. Only five adverse events were reported. After a minimum follow-up of one year for all patients, estimated event-free survival (EFS) was 93%. Z-BEAM is a safe conditioning regimen that can be used for B-cell lymphoma. Longer follow-up is necessary to evaluate long-term toxicity and efficacy.
The Z-BEAM regimen is used in other types of lymphoma, for example in those patients who are ineligible for TBI due to older age or prior radiotherapy. The group of City of Hope was a pioneer in their domain and reported their experience7 of a study of 41 patients with a median age of 60 years. Disease histology were diffuse large B-cell (n=20), mantle-cell (n=13), follicular (n=4) and transformed (n=4) lymphoma. There was a median follow-up of 18.4 months and the estimated twoyear OS and PFS were 88.9 and 69.8%, respectively.
Shimoni and others8,9 have investigated the inclusion of standard-dose 90Y–ibritumomab tiuxetan in the conditioning regimen prior to ASCT in refractory, aggressive NHL expected to have poor outcome with standard conditioning (see Table 2). Presence of active disease was determined using positron emission tomography (PET) and computed tomography (CT) scanning. Overall, 11 patients had primary refractory disease, 12 had refractory relapsed disease and 14 had bulky disease at transplant. Patients received the Z-BEAM conditioning regimen. All patients engrafted rapidly, in a median of 10 days (range 10–22 days).
Overall, 16 of 21 evaluable patients achieved a CR (76%): 11 achieved a CR, nine achieved a PR, of whom five converted to CR with additional radiation therapy to eliminate residual disease. After a median follow-up of 17 months (range six to 27 months), 16 of 23 patients were alive. Non-relapse mortality at day 100 in these heavily-pre-treated refractory patients was 9% (95% confidence interval [CI] 2–33). There was no apparent additional toxicity related to the use of 90Y–ibritumomab tiuxetan and the investigators concluded that its inclusion in this conditioning regimen was relatively safe and improved outcomes in patients with refractory lymphoma.
Escalating-dose 90Y–ibritumomab tiuxetan (0.3–1.2mCi/kg) plus high-dose BEAM was investigated in a phase I trial of relapsed or refractory CD20-positive NHL.10,11 Based on dosimetry results, patient-specific doses of 90Y–ibritumomab tiuxetan calculated to deliver escalating radiation doses (300–2,100cGy) to critical organs (liver, lung or kidney) were administered. The median age of the patients was 54 years (range 25–72 years) and most had received three or more treatment regimens, including rituximab. The toxicity profile of the 90Y–ibritumomab tiuxetan-containing conditioning regimen was similar to that seen with high-dose BEAM alone. The most common grade III or IV toxicities were infection, fever, stomatitis, nausea, vomiting, diarrhoea, haemorrhage and oedema. Engraftment was rapid and three-year OS and PFS rates were good.
Tolerability
These preliminary data indicate that 90Y–ibritumomab tiuxetan at standard- and high-/escalating-dose was well tolerated as a component of transplant-conditioning regimens. Toxicity profiles were similar to those seen with other high-dose regimens such as TBI, etoposide and cyclophosphamide, with no additional toxicity and no adverse events or allergic reactions specifically attributed to 90Y–ibritumomab tiuxetan.
Adverse events observed following 90Y–ibritumomab tiuxetan plus HDC and transplant were as expected and included skin rashes, nausea/ vomiting, mucositis, infection and cardiac, pulmonary and hepatic toxicity. In studies where 90Y–ibritumomab tiuxetan was the sole myeloablative agent, adverse events were as expected for monotherapy (neutropoenia, infections) and were relatively mild. The most frequent, severe complications normally seen with conventional HDC conditioning were not observed. Tolerability findings were similar in 131I–tositumomab studies; abnormal levels of thyroid-stimulating hormone were also frequently observed following 131I–tositumomab-based conditioning.
Conventional chemotherapy for NHL is associated with an increased risk of myelodyspalstic syndrome. This usually develops within 10 years of treatment exposure. Analysis estimated the risk of myelodysplastic syndrome or acute myeloid leukaemia in NHL patients receiving high-dose chemotherapy and ASCT to be between 5 and 10%. Clinical data for 90Y–ibritumomab tiuxetan in 746 patients reported 17 myelodysplastic syndromes, with an annualised rate of 0.7% from the time of treatment, indicating that there is no increase in risk compared with conventional chemotherapy.12
Current and Future Directions for Yttrium-90–Ibritumomab Tiuxetan in Autologous Stem Cell Transplantation
There is still a substantial need to further improve conditioning regimens in SCT through a safe treatment modality. The high relapse rates observed after ASCT suggest that most conditioning regimens are inadequate and more effective options are needed. Radiolabelled immunotherapy, in particular 90Y–ibritumomab tiuxetan, has shown great promise as part of conditioning regimens both as high-dose monotherapy and at standard- and escalated-dose alongside HDC, and appears to offer an effective and well-tolerated alternative to TBI.
Future research to evaluate the role of 90Y–ibritumomab tiuxetan alone with peripheral blood SC support should take a stepwise approach, focusing initially on phase II studies in patients with different histological NHL subtypes. Clear eligibility criteria should be included to define a homogenous population of lymphoma patients and those with a poor prognosis. Research also needs to be carried out with 90Y–ibritumomab tiuxetan as first-line therapy and following relapse. Subsequently, these results can be compared with a standard regimen in historical controls before making the decision to move on to randomised studies in poorprognosis NHL patients. ■
Z-BEAM Transplantation
Article
References
- Vignot S, Mounier N, Larghero J, et al., High-dose therapy and autologous stem-cell transplantation can improve event-free survival for indolent lymphoma: a study using patients as their own controls, Cancer, 2007;109(1):60–67.
- Weigert O, Illidge T, Hiddemann W, Dreyling M, Recommendations for the use of Yttrium-90 ibritumomab tiuxetan in malignant lymphoma, Cancer, 2006;107:686–95.
- Witzig TE, Radioimmunotherapy for B cell non-Hodgkin lymphoma, Best Pract Res Clin Haematol, 2006;19:655–68.
- Witzig TE, White CA, Gordon LI, et al., Safety of yttrium-90 ibritumomab tiuxetan radioimmunotherapy for relapsed lowgrade, follicular, or transformed non-Hodgkin’s lymphoma, J Clin Oncol, 2003;21:1263–70.
- Gisselbrecht C, Bethge W, Duarte RF, et al., Current status and future perspectives for yttrium-90 (90Y)-ibritumomab tiuxetan in stem cell transplantation for non-Hodgkin’s lymphoma, Bone Marrow Transpl, 2007;40(11):1007–17.
- Gisselbrecht C, Decaudin D, Mounier N, et al., Yttrium-90 ibritumomab tiuxetan (Zevalin) combined with BEAM (Z-BEAM) conditioning regimen plus autologous stem cell transplantation in relapsed or refractory follicular lymphoma. GELA phase II study, Blood, 2007;110(11): abstract 22.
- Krishnan A, Nademanee A, Fung HC, et al., Phase II Trial of a Transplantation Regimen of Yttrium-90 Ibritumomab Tiuxetan and High-Dose Chemotherapy in Patients With Non-Hodgkin’s Lymphoma, J Clin Oncol, 2008;26(1):90–95.
- Shimoni A, Zwass T, Oksman Y, et al., Yttrium-ibritumomab tiuxetan (Zevalin) combined with high-dose BEAM chemotherapy and autologous stem-cell transplantation for
chemo-refractory aggressive non-Hodgkin’s lymphoma, Exp Hematol, 2007;35:534–40. - Khouri IF, Saliba RM, Hosing C, et al., Efficacy and safety of Yttrium 90 (90Y) ibritumomab tiuxetan in autologous and nonmyeloablative stem cell transplantation (NST) for relapsed non- Hodgkin’s lymphoma (NHL), Blood, 2006;108: abstract 315.
- Nademanee A, Forman S, Molina A, et al., A phase 1–2 trial of high-dose yttrium-90-ibritumomab tiuxetan in combination with high-dose etoposide and cyclophosphamide followed by autologous stem cell transplantation in patients with poor-risk or relapsed non-Hodgkin lymphoma, Blood, 2005;106: 2896–2902.
- Winter JN, Inwards D, Spies S, et al., 90Y ibritumomab tiuxetan (Zevalin; 90YZ) doses calculated to deliver up to 1,500cGy to critical organs may be safely combined with high-dose BEAM and autotransplant in NHL, Blood, 2006;108: abstract 330.
- Czuczman MS, Emmanouilides C, Darif M, et al., Treatmentrelated myelodysplastic syndrome and acute myelogenous leukaemia in patients treated with ibritumomab tiuxetan radioimmunotherapy, J Clin Oncol, 2007;25(27):4285–92.
Further Resources

Trending Topic
Marginal zone lymphoma subtypes Marginal zone lymphoma (MZL) is an indolent non-Hodgkin lymphoma (NHL) that accounts for 5.0%–10.0% of NHLs.1 There are three subtypes of MZL: extranodal (including mucosa-associated lymphoid tissue [MALT]), splenic and nodal.1 Extranodal MZL (EMZL) is the most common type of MZL and accounts for about 70% of all cases of MZLs, occuring in […]
Marginal zone lymphoma subtypes Marginal zone lymphoma (MZL) is an indolent non-Hodgkin lymphoma (NHL) that accounts for 5.0%–10.0% of NHLs.1 There are three subtypes of MZL: extranodal (including mucosa-associated lymphoid tissue [MALT]), splenic and nodal.1 Extranodal MZL (EMZL) is the most ...

B-cell signalling pathways are critical regulators of B-cell development, expansion, and survival and function via various mediators, including Src family kinases (SFKs), spleen tyrosine kinase, Bruton’s tyrosine kinase (BTK) and phosphatidylinositol 3 kinase (PI3K) (Figure 1).1,2 BTK, a member of ...

The addition of rituximab to chemotherapy provides an overall survival benefit in aggressive lymphomas,1 whereas for indolent lymphoma subtypes this addition has resulted in improvements in progression-free survival.2 For more than two decades, immunotherapy with monoclonal ‘naked’ antibodies targeting CD20 ...

Allogeneic haematopoietic stem cell transplant (allo-HSCT) remains a potential curative therapeutic option for patients with refractory/relapsed Hodgkin lymphoma (HL) in whom an autologous peripheral blood stem-cell transplantation (PBSCT) has failed. This is explained by the additional benefit of a ...

Hodgkin lymphoma is a B-cell lymphoma that predominantly affects adults between 20–40 years of age, with a second incidence peak in those 55 years of age or older.1,2 It is also the most common form of lymphoma in adolescents, occurring in nearly ...

Large B-cell lymphoma includes diffuse large B-cell lymphomas, primary mediastinal B-cell lymphoma and transformed follicular lymphoma. These have historically been treated with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP). High-dose salvage chemotherapy and autologous stem-cell transplantation (SCT) can be used ...

Waldenström macroglobulinemia (WM) is an indolent lymphoma characterized by the presence of a circulating monoclonal immunoglobulin M (IgM) protein of any size and lymphoplasmacytic infiltrate in the bone marrow.1 It lies within a continuous spectrum of disorders associated with ...
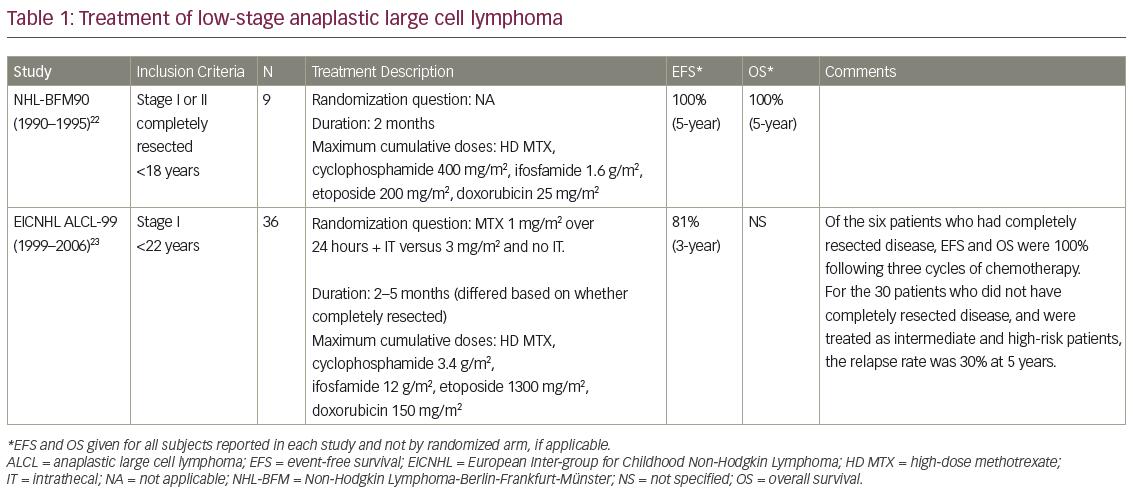
Over the course of the last three decades there has been significant improvement in the outcomes of children with non-Hodgkin lymphoma (NHL).1 However, despite varied treatment strategies and sequential clinical trials, the prognosis for one NHL subtype, anaplastic large cell ...

Post-transplant lymphoproliferative disorder (PTLD) is a severe complication of haematopoietic stem cell transplantation (HSCT). Most of the PTLDs originate from B-cells. Overall, 60–80% of PTLDs are associated with Epstein-Barr virus (EBV); this can vary depending on PTLD type and time of ...

The term paraneoplastic syndrome (PNS) was first described in the 1940s as the phenomenon that certain cancers manifest as symptoms not directly related to the tumor itself.1 Since then, there have been a multitude of reports on PNS, which is ...
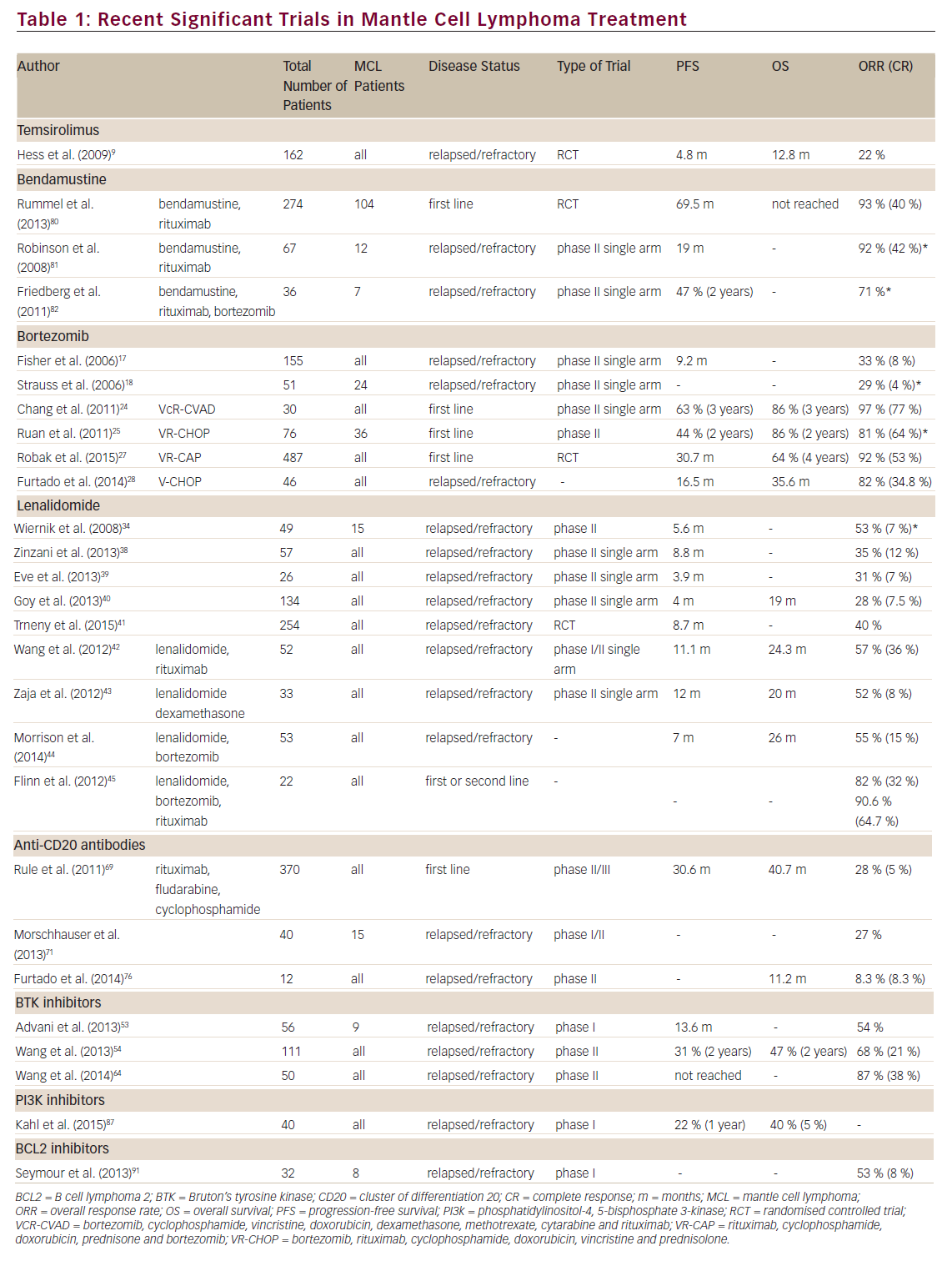
Mantle cell lymphoma (MCL) comprises ~6 % of all Non-Hodgkin lymphoma (NHL) with a median age at presentation of mid-60s. It is characterised by the t(11;14)(q13:32) translocation, which leads to overexpression of cyclin D1 resulting in subsequent dysregulation of the ...

Chemotherapy achieves excellent response rates and long progressionfree survival (PFS) in classical Hodgkin’s lymphoma (cHL) and systemic anaplastic large cell lymphoma (sALCL).1 However, up to 30 % of patients with advanced HL do not achieve remission or relapse within a few ...
Log into your Touch Account
Keep track of your clinical interests and newsletter subscriptions.
Sign up with an Email
Or use a .
Register now for FREE access
Already registered? Login below.
